Repeatedly, research have proven that medical doctors are likely to make scientific selections for sufferers primarily based on how a lot they themselves will receives a commission.
In 2007, we realized from the COURAGE trial that angioplasty and stents—percutaneous coronary intervention (PCI)—don’t scale back the danger of demise or coronary heart assault, however sufferers didn’t appear to get the memo. Just one % notice there was no mortality or coronary heart assault profit, maybe as a result of most cardiologists fail to say that truth. One can think about that if sufferers really understood that symptomatic reduction was all they have been going to get, with “no extra mortality advantages,” they’d be much less prone to go below the knife. Then, ten years later, the ORBITA trial was revealed, exhibiting even the promise of symptom reduction was an phantasm.
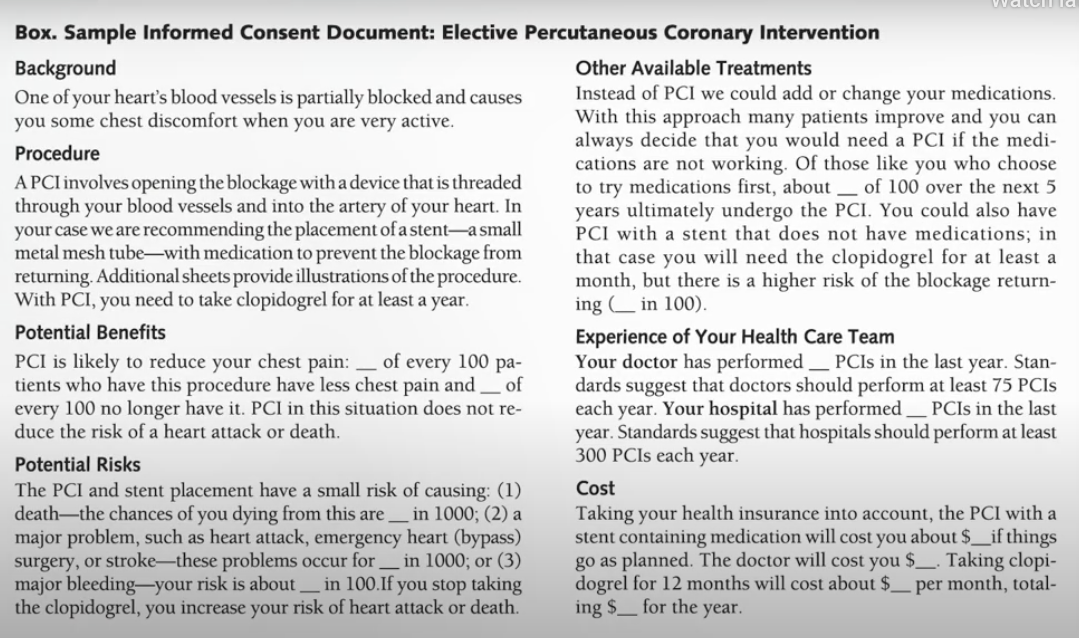
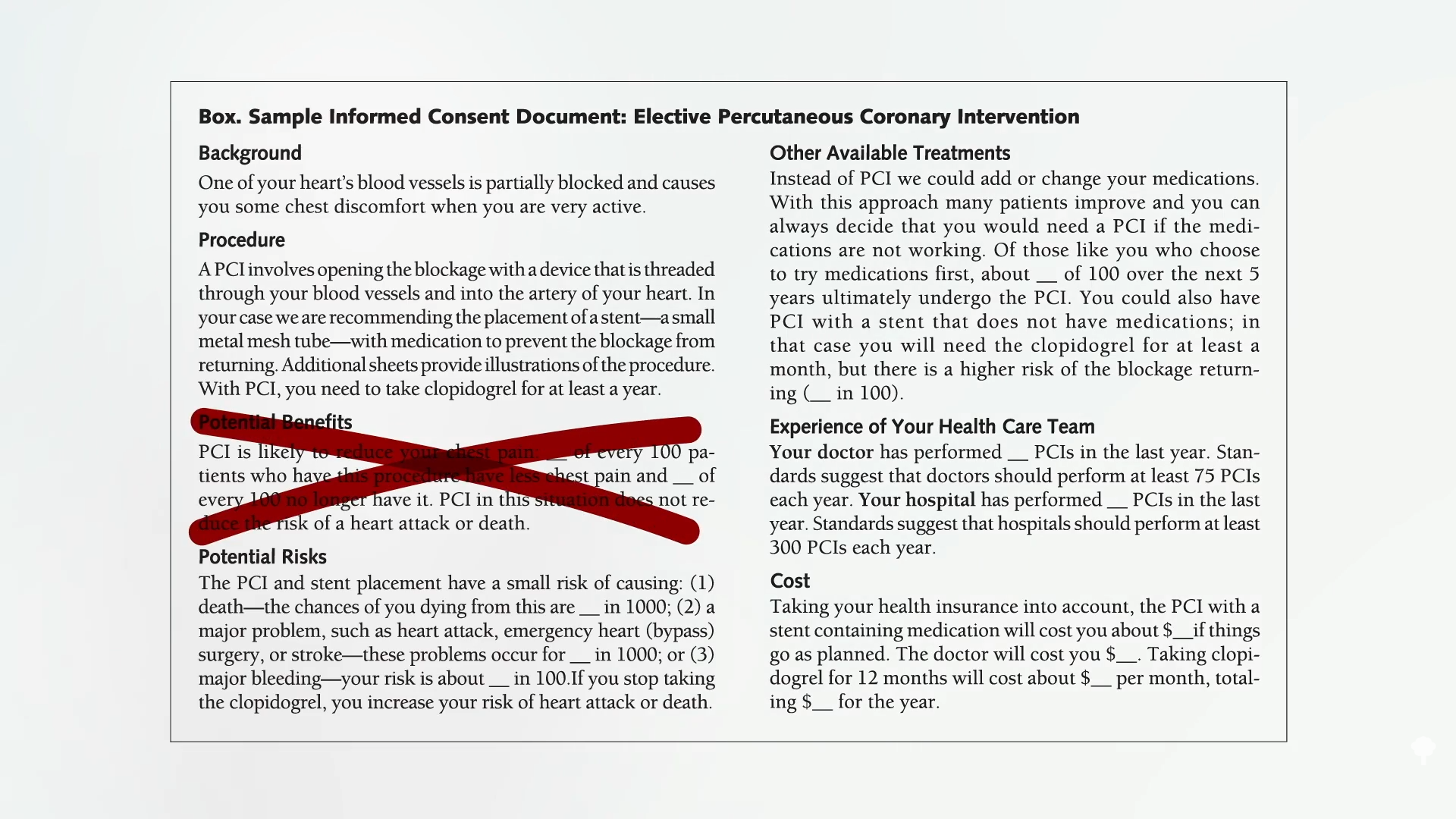
“The implications of ORBITA are profound and far-reaching. At first, the outcomes of ORBITA present unequivocally that there aren’t any advantages for PCI in contrast with medical remedy for secure angina,” that’s, coronary heart illness. Mainly, sufferers could be risking “hurt for no profit. It’s exhausting to think about a state of affairs the place a totally knowledgeable affected person would select an extra invasive remedy for no additional benefit.” Bear in mind the stent consent kind I mentioned beforehand, proven under and at 1:17 in my video Why Are Stents Nonetheless Used If They Don’t Work?:
Now, it appears like this, seen under and at 1:21.
So, is the ORBITA trial the “final nail within the coffin for PCI in secure angina?” That’s, for stents in non-emergency conditions? An editorial within the journal Cardiovascular Revascularization Medication disagreed, pointing to “the broad angina reduction that occurred in each arms.” In different phrases, stents helped—even when the sham operation with out stents helped simply as a lot. So, “if the affected person is handled with PCI and is benefiting from the ‘placebo impact,’ who am I to intervene with that benefit of this ‘remedy’?” In that case, why not carry out faux surgical procedures? Stent placement can price round $40,000. It’d be cheaper to only faux all of it. The explanation we shouldn’t hold electively stenting individuals is as a result of there’s a physique rely. Throughout stent placement, 2 % of sufferers develop bleeding or blood vessel injury, whereas one other 1 % die or have a coronary heart assault or a stroke. And since one thing is caught in your chest, 3 % of sufferers have a bleeding occasion from the blood thinners that should be taken. Or the blood thinners don’t work and the stent clots off and causes a coronary heart assault.
Why are they nonetheless accomplished once we not solely don’t have proof of profit however, in lots of circumstances, we have specific “proof of no profit”? One of many sources of resistance could also be all of the monetary acquire. These procedures make some huge cash for hospitals. Don’t count on them to start selling “life-style modifications to fight coronary heart illness. Nor will physicians shortly abandon a observe that each helps their revenue and appears to make sense.” Is it that straightforward? Is it that well-known Upton Sinclair quote: “It’s tough to get a person to know one thing when his wage relies upon upon his not understanding it.” Assume that’s simply cynicism? Let’s ask medical doctors themselves.
1000’s of physicians have been surveyed, and 70 % “believed that physicians present pointless procedures after they revenue from them.” That’s what medical doctors themselves imagine. And the info bear this out. Docs have been proven to make scientific selections for sufferers primarily based on how a lot they receives a commission. For instance, when selecting which chemotherapy to deal with breast most cancers, growing a doctor’s margin by 10 % can yield as much as a 177 % enhance within the chance of selecting one drug over one other.
That could be why Caesarean sections “usually tend to be carried out by for-profit hospitals as in contrast with non-profit hospitals.” “Working on fee.” Pay surgeons per process, and you may enhance surgical procedure charges by 78 %. May that designate why we do 101 % extra angioplasties than some other prosperous nation? A examine on “physicians’ financial incentives and remedy decisions in coronary heart assault administration” discovered that they do certainly “reply positively to the funds they obtain and that the response is sort of massive…Unconditionally, plans that pay physicians extra for extra invasive therapies are related to a bigger fraction of such therapies,” seeming to end in extra invasive therapies. So, it could really be fairly frequent for sufferers to obtain completely different therapies primarily based on whether or not the physician is getting paid per process.
One in all my heroes, Dr. Caldwell Esselstyn—who at all times tries to see the perfect in individuals—needed to admit that compensation could also be taking part in a job. Proof surfaced that “medical doctors have run up tens of millions of {dollars} in medical payments by doing pointless stent implants,” medical doctors like Mark Midei who inserted 30 stents in a single day. That may very well be about one million {dollars} value of billing. As a token of gratitude, a gross sales consultant from the stent firm spent greater than $2,000 to purchase “a complete slow-smoked pig, peach cobbler, and different fixings for a barbecue dinner at Dr. Midei’s dwelling.”
“The US is nearly the one developed nation the place well being care is delivered on a fee-per-service foundation and we very liberally incentivize physicians for doing invasive procedures,” defined the chief of cardiovascular medication on the Cleveland Clinic. “The financial incentives are simply too sturdy.”








{kind=link}
Discussion about this post